






























 Arguments
Arguments








































Positives and negatives of global warming
What the science says...
| Select a level... |
 Basic
Basic
|
 Intermediate
Intermediate
|
 Advanced
Advanced
| ||||
|
Negative impacts of global warming on agriculture, health & environment far outweigh any positives. |
|||||||
It's not bad
"By the way, if you’re going to vote for something, vote for warming. Less deaths due to cold, regions more habitable, larger crops, longer growing season. That’s good. Warming helps the poor." (John MacArthur)
At a glance
“It's not going to be too bad”, some people optimistically say. Too right. It's going to be worse than that. There are various forms this argument takes. For example, some like to point out that carbon dioxide (CO2) is plant-food – as if nobody else knew that. It is, but it's just one of a number of essential nutrients such as water and minerals. To be healthy, plants require them all.
We know how climate change disrupts agriculture through more intense droughts, raging floods or soil degradation – we've either experienced these phenomena ourselves or seen them on TV news reports. Where droughts intensify and/or become more prolonged, the very viability of agriculture becomes compromised. You can have all the CO2 in the world but without their water and minerals, the plants will die just the same.
At the same time, increased warming is adversely affecting countries where conditions are already close to the limit beyond which yields reduce or crops entirely fail. Parts of sub-Saharan Africa fall into this category. Elsewhere, many millions of people – about one-sixth of the world’s population - rely on fresh water supplied yearly by mountain glaciers through their natural melt and regrowth cycles. Those water supplies are at risk of failure as the glaciers retreat. Everywhere you look, climate change loads the dice with problems, both now and in the future.
Please use this form to provide feedback about this new "At a glance" section. Read a more technical version below or dig deeper via the tabs above!
Further details
Most climate change impacts will confer few or no benefits, but may do great harm at considerable costs. We'll look at the picture, sector by sector below figure 1.
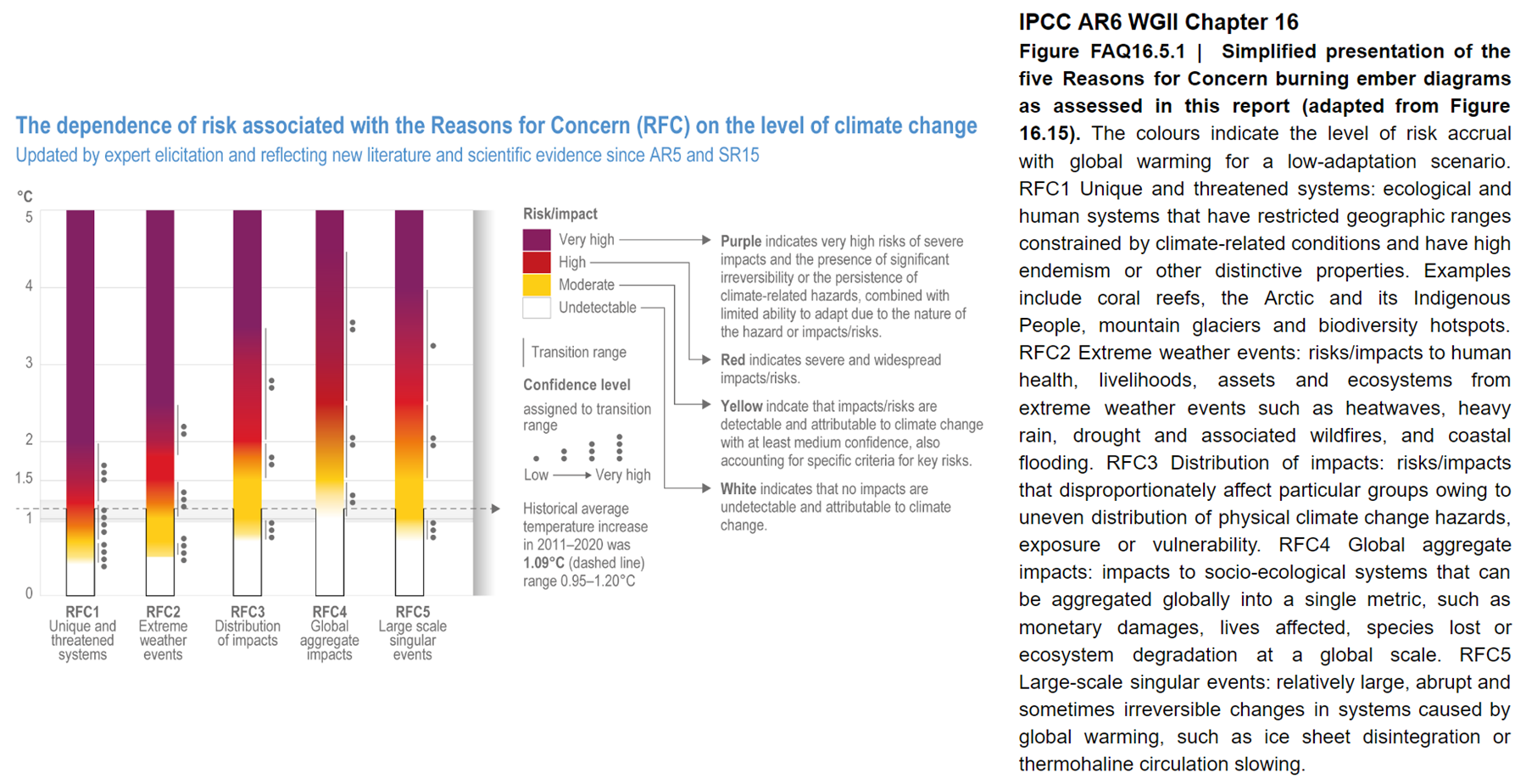
Figure 1: Simplified presentation of the five Reasons for Concern burning ember diagrams as assessed in IPCC AR6 Working Group 2 Chapter 16 (adapted from Figure 16.15, Figure FAQ 16.5.1).
Agriculture
While CO2 is essential for plant growth, that gas is just one thing they need in order to stay healthy. All agriculture also depends on steady water supplies and climate change is likely to disrupt those in places, both through soil-eroding floods and droughts.
It has been suggested that higher latitudes – Siberia, for example – may become productive due to global warming, but in reality it takes a considerable amount of time (centuries plus) for healthy soils to develop naturally. The soil in Arctic Siberia and nearby territories is generally very poor – peat underlain by permafrost in many places, on top of which sunlight is limited at such high latitudes. Or, as a veg-growing market gardening friend told us, “This whole idea of "we'll be growing grains on the tundra" is just spouted by idiots who haven't grown as much as a carrot in their life and therefore simply don't have a clue that we need intact ecosystems to produce our food.” So there are other reasons why widespread cultivation up there is going to be a tall order.
Agriculture can also be disrupted by wildfires and changes in the timing of the seasons, both of which are already taking place. Changes to grasslands and water supplies can impact grazing and welfare of domestic livestock. Increased warming may also have a greater effect on countries whose climate is already near or at a temperature limit over which yields reduce or crops fail – in parts of the Middle East and sub-Saharan Africa, for example.
Health
Warmer winters would mean fewer deaths, particularly among vulnerable groups like the elderly. However, the very same groups are also highly vulnerable to heatwaves. On a warmer planet, excess deaths caused by heatwaves are expected to be approximately five times higher than winter deaths prevented.
In addition, it is widely understood that as warmer conditions spread polewards, that will also encourage the migration of disease-bearing insects like mosquitoes, ticks and so on. So long as they have habitat and agreeable temperatures to suit their requirements, they'll make themselves at home. Just as one example out of many, malaria is already appearing in places it hasn’t been seen before.
Polar Melting
While the opening of a year-round ice-free Arctic passage between the Atlantic and Pacific oceans would have some commercial benefits, these are considerably outweighed by the negatives. Detrimental effects include increased iceberg hazards to shipping and loss of ice albedo (the reflection of sunshine) due to melting sea-ice allowing the ocean to absorb more incoming solar radiation. The latter is a good example of a positive climate feedback. Ice melts away, waters absorb more energy and warming waters increase glacier melt around the coastlines of adjacent lands.
Warmer ocean water also raises the temperature of submerged Arctic permafrost, which then releases methane, a very potent greenhouse gas. The latter process has been observed occurring in the waters of the East Siberian Arctic Shelf and is poorly understood. At the other end of the planet, melting and break-up of the Antarctic ice shelves will speed up the land-glaciers they hold back, thereby adding significantly to sea-level rise.
Ocean Acidification
Acidity is measured by the pH scale (0 = highly acidic, 7 = neutral, 14 = highly alkaline). The lowering of ocean pH is a cause for considerable concern without any counter-benefits at all. This process is caused by additional CO2 being absorbed in the water. Why that's a problem is because critters that build their shells out of calcium carbonate, such as bivalves, snails and many others, may find that carbonate dissolving faster than they can make it. The impact that would have on the marine food-chain should be self-evident.
Melting Glaciers
The effects of glaciers melting are largely detrimental and some have already been mentioned. But a major impact would be that many millions of people (one-sixth of the world’s population) depend on fresh water supplied each year by the seasonal melt and regrowth cycles of glaciers. Melt them and those water supplies, vital not just for drinking but for agriculture, will fail.
Sea Level Rise
Many parts of the world are low-lying and will be severely affected even by modest sea level rises. Rice paddies are already becoming inundated with salt water, destroying the crops. Seawater is contaminating rivers as it mixes with fresh water further upstream, and aquifers are becoming saline. The viability of some coastal communities is already under discussion, since raised sea levels in combination with seasonal storms will lead to worse flooding as waves overtop more sea defences.
Environmental
Positive effects of climate change may include greener rainforests and enhanced plant growth in the Amazon, increased vegetation in northern latitudes and possible increases in plankton biomass in some parts of the ocean.
Negative responses may include some or all of the following: further expansion of oxygen-poor ocean “dead zones”, contamination or exhaustion of fresh water supplies, increased incidence of natural fires and extensive vegetation die-off due to droughts. Increased risk of coral extinction, changes in migration patterns of birds and animals, changes in seasonal timing and disruption to food chains: all of these processes point towards widespread species loss.
Economic
Economic impacts of climate change are highly likely to be catastrophic, while there have been very few benefits projected at all. As long ago as 2006, the Stern Report made clear the overall pattern of economic distress and that prevention was far cheaper than adaptation.
Scenarios projected in IPCC reports have repeatedly warned of massive future migrations due to unprecedented disruptions to global agriculture, trade, transport, energy supplies, labour markets, banking and finance, investment and insurance. Such disturbances would wreak havoc on the stability of both developed and developing nations and they substantially increase the risk of future conflicts. Furthermore, it is widely accepted that the detrimental effects of climate change will be visited mostly on those countries least equipped to cope with it, socially or economically.
These and other areas of concern are covered in far more detail in the 36-page Summary for Policymakers from the IPCC AR6 Synthesis Report, released in March 2023. The report spells out in no uncertain terms the increasingly serious issues Mankind faces; the longer that meaningful action on climate is neglected, the greater the severity of impacts. The report is available for download here.
Last updated on 21 April 2023 by John Mason. View Archives




Climate Myth...